Lumbar Puncture (spinal tap) is a diagnostic and at times therapeutic procedure that is performed in order to collect a sample of cerebrospinal fluid (CSF) for biochemical, microbiological, and cytological analysis, or very rarely as a treatment (“therapeutic Lumbar Puncture”) to relieve increased intracranial pressure.
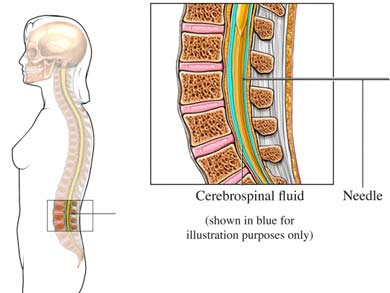
In performing a Lumbar Puncture, the patient is seated on the examination table and is asked to bend his/her head and shoulders forward. The area around the lower back is prepared using aseptic technique. Once the appropriate location is palpated, local anesthetic is infiltrated under the skin and then injected along the intended path of the spinal needle. A spinal needle is inserted between the lumbar vertebrae L3/L4 or L4/L5 and pushed in until there is a “give” that indicates the needle is past the dura mater. The stylet from the spinal needle is then withdrawn and 12 ml of cerebrospinal fluid are collected. The opening pressure is not routinely measured for neuromuscular indications. The procedure is ended by withdrawing the needle while placing pressure on the puncture site. In the past, the patient would often be asked to lie on his/her back for at least six hours and be monitored for signs of neurological problems, though there is no scientific evidence that this provides any benefit. The technique described is almost identical to that used in spinal anesthesia, except that spinal anesthesia is more often done with the patient in a sitting position.
Oral anticoagulant such as warfarin are preferably stopped 5 days before the procedure and resumed right after it if permitted by the prescribing physicians.
About 25 ml of CSF is produced /hour in a normal individual, which is enough to replace the entire CSF volume (150 ml) three times a day. The collected fluid is replenished within an hour but sometimes continuing leak of CSF from a dural tear lead to severe postural headache after the procedure which usually resolves within a week but if continues a blood patch usually gives dramatic resolution.
Elevation of the CSF protein, in particular the IgG synthesis rate and IgG index, suggests an inflammatory process such as inflammatory neuropathy. Significant elevation of the CSF protein is an important diagnostic criterion of CIDP.